How to Perform a Cardiac Auscultation
Basics of Auscultation
Auscultation of a heart begins with two critical items: a stethoscope and a patient. Knowledge about both these elements is key to assessing the health of a heart. Classic stethoscopes have two sides of the chestpiece—the diaphragm and the bell. The larger, flatter side is the diaphragm and is used for listening to higher-pitched sounds. The bell is the smaller, concave side that allows for auscultation of lower-pitched sounds like some heart murmurs. When performing a cardiac exam, auscultation should be performed with the diaphragm and then repeated with the bell.
Heart Valves
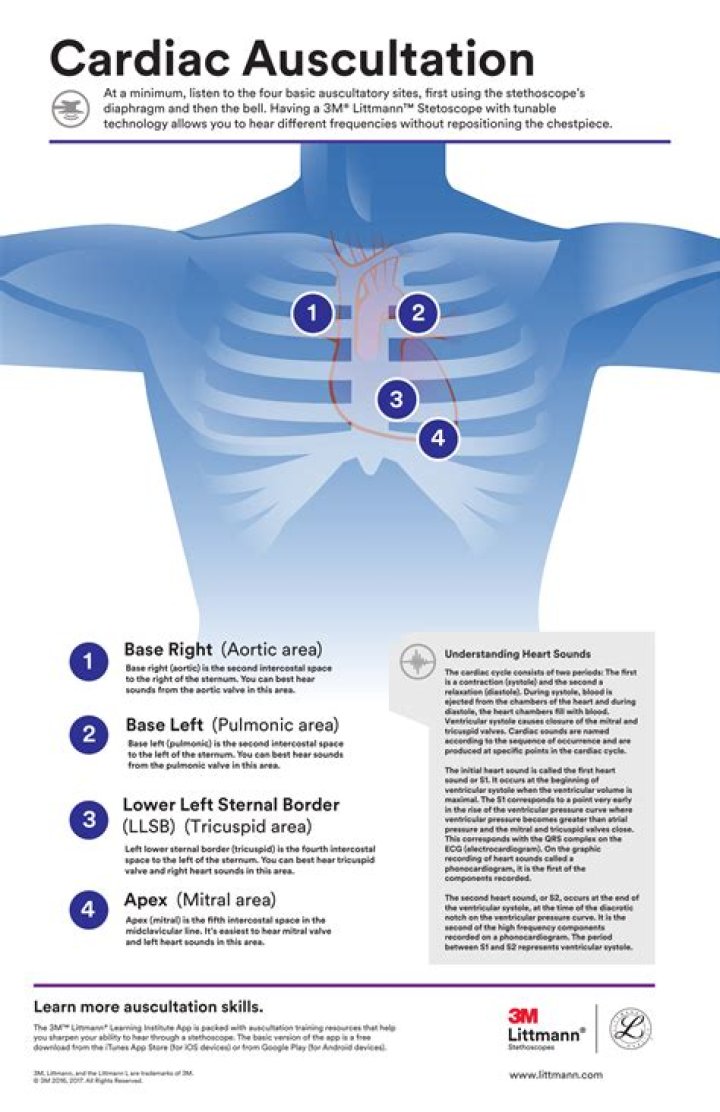
The locations of auscultation center around the heart valves. The aortic, pulmonic, tricuspid, and mitral valves are four of the five points of auscultation. The fifth is Erb’s point, located left of the sternal border in the third intercostal space. The aortic point is located right of the sternal border in the second intercostal space. The pulmonic point is to the left of the sternal border in the second intercostal space. The sound that emits from the aortic and pulmonic points is the S2 “dub” of the typical “lub-dub” heartbeat. The S1 and S2 sounds are present in normal heartbeat patterns.
The tricuspid point is found left of the sternal border in the fourth intercostal space, and the mitral point is located midclavicular on the left side of the chest in the fifth intercostal space. Both the tricuspid and the mitral points are where the S1 “lub” can be heard. The base of the heart is where the aortic and pulmonic S2 sound will be loudest. The apex is where the tricuspid and mitral S1 sound is loudest upon auscultation. The apex region will also be where S3 and S4 sounds(extra heart sounds not usually noted in normal assessments) and mitral stenosis murmurs may be auscultated, if present.
Mnemonic device
A mnemonic that aids in recalling the points of auscultation is APE To Man:
Patient positioning during assessment facilitates the auscultation of various valve anomalies. Initially, a complete auscultation assessment should be performed as the patient is in supine or sitting position. Then, patients should be positioned laterally onto their left side so the provider can listen with the bell of the stethoscope for any S3, S4 (extra heart sounds) and/or mitral stenosis murmurs in the apex region. Aortic and pulmonic murmurs are more easily identified with the diaphragm of the stethoscope when patients are in a sitting position, leaned forward, and asked to exhale.
It is important to perform a comprehensive assessment of the heart, listening to all five points and keeping in mind which side of the chestpiece should be utilized during listening, as well as the patient’s position during auscultation.
In this video, doctors can learn how to perform a full cardiac examination on a patient. The very first thing a doctor should do is visually inspect the patient, because there’s a lot that can be gained by simply examining by eye. You’ll want to carefully examine the respiratory pattern of the patient, the nature of their precordium, the anterior part of their chest over the heart. Feeling the pulse is also necessary when starting out this heart exam. To learn more, watch the full video.
For a full lesson on cardiac examination, go to University of Virginia’s School of Medicine Interactive Learning Module. The best way to prepare yourself for your small group exercises is to first watch the cardiac exam video from beginning to end, then proceed through all the explanations of cardiac anatomy and physiology that are in the lesson. By the end of this session, you will be able to:
1. Recognize the elements and significance of the jugular venous pulse.
2. Know the physiology and sound of S1 and S2.
3. Know the physiology and sound of S3 and S4.
4. Identify systole and diastole by palpation and listening.
5. Describe heart murmurs.
6. Hear and understand the mechanism of three common systolic murmurs.
Want to master Microsoft Excel and take your work-from-home job prospects to the next level? Jump-start your career with our Premium A-to-Z Microsoft Excel Training Bundle from the new Gadget Hacks Shop and get lifetime access to more than 40 hours of Basic to Advanced instruction on functions, formula, tools, and more.
During the nursing head-to-toe assessment, the nurse will be listening to the heart with a stethoscope. Auscultating the heart allows the nurse to assess the heart’s rhythm, rate, and sound of valve closure. The nurse will be assessing S1 and S2 while noting if there are any S1 and S2 splits or extra heart sounds like S3, S4, or heart murmurs.
It is very important you are able to understand how to distinguish between S1 and S2 and what S3, S4, and heart murmurs sound like. Please see the article on “Heart Sounds Explained” for an in depth explanation on heart sounds.
In this article, you will learn how to perform an assessment of the heart. Please watch the video below for a demonstration for stethoscope placement and patient positioning.
How to Listen to the Heart with a Stethoscope
Tips for Heart Auscultation
Remember the mnemonic “All Patients Take Medicine”
Aortic: found right of the sternal border in the 2nd intercostal space REPRESENTS S2 “dub”
Pulmonic: found left of the sternal border in the 2nd intercostal space REPRESENTS S2 “dub”
Erb’s Point: found left of the sternal border in the 3rd intercostal space
Tricuspid: found right of the sternal border in the 4th intercostal space REPRESENTS S1 “lub”
Mitral: found midclavicular in the 5th intercostal space REPRESENTS S1 “lub” (also the site of point of maximal impulse)
The Base of the heart includes the aortic and pulmonic areas, and S2 will be loudest at the base. Aortic and pulmonic murmurs are heard best at the base with the patient leaning forward and sitting up with the diaphragm of the stethoscope.
The Apex of the heart includes the tricuspid and mitral areas, and S1 will be loudest at the apex. S3 and S4 along with mitral stenosis murmurs will be heard best at this position with the patient lying on their left side with the bell of the stethoscope.
Patient Positioning for Heart Auscultation
Supine or sitting-up: Use the diaphragm and listen at all 5 auscultation sites (noting S1 and S2 and if there are any splits presents). In addition, distinguish S1 from S2. Then repeat with the bell of the stethoscope…noting any other extra sounds.
Left side: turn the patient onto their left side and auscultate with the bell of the stethoscope at the APEX area and listen for S3, S4, or mitral stenosis murmurs.
Sit up, lean forward, and have patient exhale: Listen with the diaphragm at the aortic and pulmonic sites for murmurs.
You may be interested in “Heart Sounds Quiz“
Key principles for a successful exam:
- Develop a systematic approach.
- Listen selectively and specifically. Certain cardiac sounds must be “tuned out” (e.g. murmurs) while listening specifically to others (e.g. first and second heart sounds).
- Identify the timing of sounds in relation to the cardiac cycle.
- Understand and utilize patient positioning and respiratory maneuvers to evaluate findings.
Timing of auscultatory findings:
At heart rates under 120, diastole is longer than systole. At these rates it is fairly easy for the listener to identify S1 and S2, with systole being between them, and pairs of grouped S1s and S2s being separated by the longer diastolic interval. Identifying S1 and S2 correctly (and therefore systole and diastole) is imperative for correctly identifying the timing of other sounds/murmurs in the cardiac cycle.
With heart rates over 120, and with certain arrythmias, the duration of systole and diastole become indistinguishable. The timing of auscultatory sounds must therefore be determined by correlation with the carotid or apical impulse both of which occur in early systole just after S1.
Exam sequence and auscultation in the supine position:
Initially, auscultation should be conducted with the patient in the supine position, the head of the bed raised 15-30 degrees and the diaphragm of the stethoscope pressed firmly against the chest wall. Normal findings have been derived from this position. All other positions are considered “maneuvers” to further identify cardiac pathology. Auscultation should proceed in a systematic fashion from either apex to base or vice versa, as described in the video segment below.
| Click on the video icon to view a demonstration and discussion of auscultation in the supine position. |
The left lateral decubitus and upright position:
After the initial cardiac evaluation, patients should be examined in the left lateral decubitus position with the diaphragm and bell of the stethoscope. With the patient in this position, the examiner should listen specifically and selectively for a left-sided S3 or S4, and the diastolic rumble of mitral stenosis. These sounds may be found only in this position and heard only with the bell.
Auscultation of the Chest
Note the quality of the first and second heart sounds at each site, and whether there are any additional sounds. The first heart sound has two components, caused by mitral and tricuspid valve closure. Mitral closure occurs slightly before tricuspid but this does not normally cause splitting of the sound. The second heart sound is a slightly lower pitch than the first, it occurs at the end of systole. It comprises both aortic and pulmonary valve closure. A useful mnemonic is that the valves close in alphabetical order, i.e. aortic before pulmonary and mitral before tricuspid.
During inspiration, splitting of the second sound may be detected over the pulmonary area: this is due to the increased venous return to the right ventricle, leading to more prolonged systole on the right side of the heart. Splitting of the first heart sound may indicate complete right bundle branch block, whereas increase of the normal splitting of the second heart sound occurs if there is delay in right ventricular emptying, as in right bundle branch block, pulmonary stenosis, ventricular septal defects and mitral incompetence.
Atrial septal defects typically cause a fixed splitting of the second sound. Reverse splitting of the second sound (i.e. splitting occurring in expiration, as opposed to inspiration) is due to delayed left ventricle depolarization (e.g. left bundle branch block) and delayed left ventricular emptying (e.g. aortic stenosis, coarctation of the aorta and patent ductus arteriosus).
Auscultation starts over the apex, where the mitral valve is assessed. In this mitral area, apply the bell of the stethoscope (figure 51a). It produces a resonating chamber that is particularly efficient in amplifying the low pitched sounds, that may occur with mitral diastolic murmurs and a fourth heart sound.
Affiliations
- 1 Division of Cardiology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam-si, Republic Of Korea.
- 2 School of Computing, Korea Advanced Institute of Science and Technology, Daejeon, Republic Of Korea.
- 3 Division of Cardiology, Cardiovascular Center, Seoul National University Bundang Hospital, Seongnam-si, Republic Of Korea.
- PMID: 29490899
- PMCID: PMC5853766
- DOI: 10.2196/mhealth.8946
Free PMC article
- Search in PubMed
- Search in NLM Catalog
- Add to Search
Authors
Affiliations
- 1 Division of Cardiology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam-si, Republic Of Korea.
- 2 School of Computing, Korea Advanced Institute of Science and Technology, Daejeon, Republic Of Korea.
- 3 Division of Cardiology, Cardiovascular Center, Seoul National University Bundang Hospital, Seongnam-si, Republic Of Korea.
- PMID: 29490899
- PMCID: PMC5853766
- DOI: 10.2196/mhealth.8946
Abstract
Background: Cardiac auscultation is a cost-effective, noninvasive screening tool that can provide information about cardiovascular hemodynamics and disease. However, with advances in imaging and laboratory tests, the importance of cardiac auscultation is less appreciated in clinical practice. The widespread use of smartphones provides opportunities for nonmedical expert users to perform self-examination before hospital visits.
Objective: The objective of our study was to assess the feasibility of cardiac auscultation using smartphones with no add-on devices for use at the prehospital stage.
Methods: We performed a pilot study of patients with normal and pathologic heart sounds. Heart sounds were recorded on the skin of the chest wall using 3 smartphones: the Samsung Galaxy S5 and Galaxy S6, and the LG G3. Recorded heart sounds were processed and classified by a diagnostic algorithm using convolutional neural networks. We assessed diagnostic accuracy, as well as sensitivity, specificity, and predictive values.
Results: A total of 46 participants underwent heart sound recording. After audio file processing, 30 of 46 (65%) heart sounds were proven interpretable. Atrial fibrillation and diastolic murmur were significantly associated with failure to acquire interpretable heart sounds. The diagnostic algorithm classified the heart sounds into the correct category with high accuracy: Galaxy S5, 90% (95% CI 73%-98%); Galaxy S6, 87% (95% CI 69%-96%); and LG G3, 90% (95% CI 73%-98%). Sensitivity, specificity, positive predictive value, and negative predictive value were also acceptable for the 3 devices.
Conclusions: Cardiac auscultation using smartphones was feasible. Discrimination using convolutional neural networks yielded high diagnostic accuracy. However, using the built-in microphones alone, the acquisition of reproducible and interpretable heart sounds was still a major challenge.
Trial registration: ClinicalTrials.gov NCT03273803; (Archived by WebCite at ).
Keywords: cardiac auscultation; mobile health care; physical examination; smartphone; telemedicine.
Normal gut sounds may be audible even without a stethoscope, particularly after meals and with hunger. At other times sounds may be remarkably few, occurring up to every 10 seconds. These borborygmi (gurgles) can be best heard by placing the stethoscope on each side of the umbilicus. The sounds are markedly accentuated in intestinal obstruction, particularly during the contractions of colic. They are also increased by irritation from blood in the bowel or in any form of diarrhea.
Excess fluid in the gut, as for example in pyloric stenosis, may splash around when the abdomen in gently shaken by holding either side of the pelvis. This succussion splash may also be present two to three hours after a meal. It may be audible without a stethoscope. If not, ask the patient to hold the instrument in position, while you use both hands to shake the abdomen from side to side.
Paralyzed gut (paralytic ileus), such as postoperatively or in generalised peritonitis, is silent. But listen intently for a few minutes (figure 49a,b). In the late stages of intestinal obstruction, the gut may be markedly dilated and atonic, with few gut sounds, but with marked hyper- resonance (a condition known as tympanitic) and tinkling sounds of fluid dripping from one distended loop to another. In complete paralysis, breath and heart sounds may be clearly audible over the abdomen. In established obstruction a large amount of fluid accumulates in the gut, this can be shown on a plain radiograph as fluid levels. An occasional level may be seen normally, but many horizontal lines are present in obstruction; the patient can be sitting or standing, or lying on their side (figure 50).
Monitor bodily sounds & heart
Emre Turgay
- 4.0 • 136 Ratings
- Free
- Offers In-App Purchases
Screenshots
Description
This app captures and displays bodily sounds using the built-in microphone of your device.
The sound signal is displayed both in time domain and in frequency domain in real time.
There is a list of previously recorded hearth sounds that you can play, listen and visualize using the spectrogram and time domain graphical interface. Improve your knowledge and skill at identifying various conditions.
You can also visualize your own heart waveform. You can record, playback and share your own sound files with your friends.
There is a heart sound simulator by which you create various conditions. Different types of murmur, click sounds, lung sounds etc.
The captured sound is processed and filtered for best visual and audio experience. You can also control filter parameters live. The spectrogram of the sound is also displayed in real time.
Using with Airpods:
* Put on your airpods
* Press the microphone at the bottom of your device to your chest.
* Place the microphone directly against the skin, a good spot is the apex of your heart just below your left nipple.
Using with headphones:
* Press the mute button on the app interface to stop microphone feedback.
* Press the microphone at the bottom of your device to your chest.
* Place the microphone directly against the skin, a good spot is the apex of your heart just below your left nipple.
* Start recording.
* Go to playback mode and listen to your own heart beat using your HEADPHONES.
This program is not meant for diagnosis of any medical condition. The data provided can be inaccurate and should only be used for entertainment purposes. This app records and playbacks recorded sound just like any other sound recording app. The quality or validity of the recorded sound is strictly limited to the performance of the built in microphone.
This app offers premium membership. By subscribing you will get:
* Access the full library
* Access frequency domain views.
* Able to save more than one recording.
- Module 1: About canine heart disease
- Module 1
- Prevalence of heart disease
- Types of heart disease
- Progression of heart disease
- Common signs of heart failure
- Review
- Module 1
- Module 2: Diagnosis of canine heart failure
- Module 2
- Signalment
- Clinical history
- Physical examination
- Cardiac and pulmonary auscultation
- Thoracic radiographs
- Other diagnostic tests
- Review
- Module 2
- Module 3: Treatment of canine heart failure
- Module 3
- Goals of therapy
- Rationale for medications
- Types of medications
- Review
- Module 3
Cardiac and pulmonary auscultation (continued)
A useful technique is to place your hands on both sides of the dog’s chest before listening with a stethoscope. Search for where the heart is actually beating or pulsating. It is usually about halfway between the shoulder and elbow and should rest under your middle two fingers as in the first photograph below. This precordial impulse comes from the apex of the heart and is aligned with the mitral valve.
Click here to view the proper location to listen to a dog’s heart.
Click here to view a diagram of the location of a dog’s heart valves.
It is helpful to know that if you suspect a possible congenital abnormality, abnormal sounds are more likely to be heard dorsally on the thoracic wall closer to the heart base, not at the location of the precordial impulse.
- Medical Editor: William C. Shiel Jr., MD, FACP, FACR
What are heart sounds?
Heart sounds are generated by blood flowing in and out of the heart’s chambers through the valves as they open and close. Listening to the heart sounds through a stethoscope (auscultation) is one of the first steps a physician takes in evaluating a patient’s medical condition.
Heart sounds provide the doctor valuable information about heart function. Auscultation is used to detect abnormal heart sounds and decide on further course of action.
How does the heart function?
The heart is a muscular organ and has four chambers that receive and pump blood:
- Right atrium
- Right ventricle
- Left atrium
- Left ventricle
- The left atrium receives oxygenated blood from the lungs and pumps it into the left ventricle.
- The left ventricle pumps the oxygen-rich blood to the rest of the body through a network of arteries.
- The right atrium receives the oxygen-depleted blood from the body through veins and pumps it into the right ventricle.
- The right ventricle pumps the blood to the lungs for oxygenation.
The left ventricle’s contractions while pumping out blood create the systolic blood pressure in the arteries (the higher number in a blood pressure reading). A web of nerve tissue runs through the heart to send electric signals to the heart muscle to initiate the heart’s contraction.
Heart valves ensure that the flow of the blood is in only one direction, by opening and closing as the heart pumps blood. The four heart valves are
- Tricuspid valve separating right atrium and right ventricle
- Mitral valve separating left atrium and ventricle
- Pulmonic valve between right ventricle and pulmonary artery
- Aortic valve between the left ventricle and aorta
What creates the heart sounds?
Blood flow creates vibrations in the heart chambers and valves which produce audible sounds that can be heard through a stethoscope. Smooth, low-resistance blood flow is called a laminar flow. When the flow is rough with high resistance it is known as a turbulent flow.
Vibrations increase along with blood flow turbulence and depend on the diameter of the blood vessel as well as the blood’s
- viscosity
- density
- velocity
Some of the functions of the heart that generate heart sounds are
- Opening or closing of the heart valves
- Flow of blood through the valve opening
- Flow of blood into the heart’s ventricles
- Rubbing of cardiac surfaces
What are the four heart sounds?
The cardiac cycle is made of two phases:
- Systole while the ventricles contract to pump out blood
- Diastole when the ventricles relax and fill with blood.
These two phases constitute the heartbeat.
In a healthy adult, the heart makes two sounds, commonly described as ‘lub’ and ‘dub.’
The third and fourth sounds may be heard in some healthy people, but can indicate impairment of the heart function. S1 and S2 are high-pitched and S3 and S4 are low-pitched sounds.
First sound
When the two ventricles contract and pump out blood into the aorta and pulmonary artery the mitral and tricuspid valves close to prevent the blood flowing back into the atria. The first sound S1 is generated by vibrations created by the closing of these two valves.
Normally the mitral valve closes just before the tricuspid valve, and when the two different sounds are detectable, it is called a “split S1.” A split S1 may be indicative of certain conditions affecting the heart.
Second sound
After pumping the blood, the ventricles relax to receive blood from the atria, and the diastole phase starts. The aortic and pulmonic valves close and cause vibrations, giving rise to the second heart sound, S2. The increase in intensity of this sound may indicate certain conditions.
When the aortic valve closes just before the pulmonic valve, it may generate a split S2. This may indicate impairment in the heart function.
Third sound
The third heart sound is a low-pitched sound audible with the rapid rush of blood from the atrium into the ventricle as it starts relaxing. This may be a normal sound in some people but in people with heart conditions, S3 may indicate heart failure.
Fourth sound
The fourth is a low-intensity sound heard just before S1 in the cardiac cycle. The sudden slowing of blood flow by the ventricle as the atrium contracts causes this sound, which may be a sign of heart disease.
SLIDESHOW
Other heart sounds
Opening snap
Opening snap (OS) is a high-pitched sound that is caused by rapid opening of the mitral or tricuspid valve following the aortic valve closing sound (S2). This may indicate narrowing (stenosis) of the mitral or tricuspid valve; the closer in time the OS is to S2, the more severe the stenosis.
Ejection systolic sounds
These sounds are heard during the early part of the ventricular contraction, which may be
- Valvular ejection sounds due to defects in the aortic or pulmonic valves
- Vascular ejection sounds due to defects of the aortic or pulmonary artery
- Nonejection systolic click due to mitral or tricuspid valve prolapse
Heart murmurs
In some people, heart murmurs are just the sound of blood flow characteristic to that person. Doctors call this an “innocent heart murmur.” Heart murmur may also be caused by turbulent flow of blood across the heart valves, however, which may indicate heart disease.
In this Article
In this Article
In this Article
- Wheezing
- Crackling (Rales)
- Stridor
- Rhonchi
- Whooping
- Pleural Friction Rub
- Mediastinal Crunch
- Tests
If your doctor thinks you might have an issue with your lungs, the type and location of certain breathing sounds can help them figure out what might be behind it.
Wheezing
This high-pitched whistling noise can happen when you’re breathing in or out. It’s usually a sign that something is making your airways narrow or keeping air from flowing through them.
Two of the most common causes of wheezing are lung diseases called chronic obstructive pulmonary disease (COPD) and asthma. But many other issues can make you wheeze, too, including:
- Allergies
- Bronchitis or bronchiolitis
- Emphysema
- Epiglottitis (swelling of the top flap of your windpipe)
- Gastroesophageal reflux disease (GERD)
- Heart failure
- Lung cancer
- Sleep apnea
- Pneumonia
- Respiratory syncytial virus (RSV)
- Vocal cord problems
- An object stuck in your voice box or windpipe
You can also start wheezing if you smoke or as a side effect of some medications. It’s not always serious, but if you have trouble breathing, are breathing really fast, or your skin turns a bluish color, see your doctor.
If you start wheezing suddenly after an insect bite or after eating food you may be allergic to, go to the emergency room right away.
Crackling (Rales)
This is a series of short, explosive sounds. They can also sound like bubbling, rattling, or clicking. You’re more likely to have them when you breathe in, but they can happen when you breathe out, too.
You can have fine crackles, which are shorter and higher in pitch, or coarse crackles, which are lower. Either can be a sign that there’s fluid in your air sacs.
They can be caused by:
- Pneumonia
- Heart disease
- Pulmonary fibrosis
- Cystic fibrosis
- COPD
- Lung infections, like bronchitis
- Asbestosis, a lung disease caused by breathing in asbestos
- Pericarditis, an infection of the sac that covers your heart
Stridor
This harsh, noisy, squeaking sound happens with every breath. It can be high or low, and it’s usually a sign that something is blocking your airways. Your doctor can typically tell where the problem is by whether your stridor sounds happen when you breathe in or out. It’s not always serious, but it sometimes can be a sign of a life-threatening problem that needs medical attention right away.
Continued
You may get stridor if you have:
- Laryngomalacia (softening of the vocal cords in babies)
- Paralyzed vocal cord
- Narrow voice box
- Unusual growth of blood vessels (hemangioma) just below your vocal cords
- Croup
- Infection of your trachea (windpipe)
- Epiglottitis (when the “lid” of cartilage that covers your windpipe swells and blocks the flow of air to your lungs)
You can also have stridor if an object gets stuck in your windpipe. You might need surgery to fix that problem.
Rhonchi
These low-pitched wheezing sounds sound like snoring and usually happen when you breathe out. They can be a sign that your bronchial tubes (the tubes that connect your trachea to your lungs) are thickening because of mucus.
Rhonchi sounds can be a sign of bronchitis or COPD.
Whooping
This high-pitched gasp typically follows a long bout of coughing. If you hear a “whoop” when you breathe in, it may be a symptom of whooping cough (pertussis), a contagious infection in your respiratory system.
Pleural Friction Rub
The membranes that cover the walls of your chest cavity and the outer surface of your lungs are called pleura. If they get inflamed and rub together, they can make this rough, scratchy sound.
It can be a sign of pleurisy (inflammation of your pleura), pleural fluid (fluid on your lungs), pneumonia, or a lung tumor.
Mediastinal Crunch
This sound, also called Hamman’s sign, tells your doctor that air is trapped in the space between your lungs (called the mediastinum). It’s a crunchy, scratchy sound, and it happens in time with your heartbeat. That’s because your heart movements shift the trapped air and cause the scratching sounds.
These crunching sounds can sometimes mean you have a collapsed lung, especially if you also have chest pain and shortness of breath. They also can be a sign of lung disease like COPD, pneumonia, or cystic fibrosis.
Tests
Your doctor can get important information about the health of your lungs by listening closely as you breathe. The easiest and most common way to do this is to hold a stethoscope to the skin on your back and chest. This is called auscultation.
Continued
As your doctor listens, they’ll ask you to take deep breaths through your mouth. They also may ask you to speak certain phrases and see how they sound through your chest or back. Some examples of this include:
- Bronchophony: Your doctor will ask you to say “ninety-nine.” Normally, your lungs will muffle the words. If the words sound clear through the stethoscope, it may be a sign that your lungs are filled with blood, fluid, or mucus.
- Whispered pectoriloquy: This involves whispering “ninety-nine” or “one, two, three.” Healthy lungs will dampen the sound and make the words faint, but they’ll be louder if your lungs are filled with fluid.
- Egophony: If you have fluid in your lungs, your doctor uses this test to check for a collapsed lung. As you say an “e” sound, your doctor will listen to see if it’s muffled and sounds like “e” or if it’s louder and sounds like “a,” which means fluid is changing the sound.
Sources
Annals of Thoracic Medicine: “Auscultation of the respiratory system.”
PLOS One: “Automatic adventitious respiratory sound analysis: A systematic review.”
Mayo Clinic: “Wheezing,” “Whooping cough,” “Pneumothorax.”
Medscape: “Breath Sound Assessment,” “Pneumomediastinum.”
Cleveland Clinic: “Pericarditis.”
American Family Physician: “Diagnosis of Stridor in Children.”
Stanford Children’s Health: “Stridor.”
U.S. National Library of Medicine: “Pleurisy and Other Pleural Disorders.”
Schilling, J. Evaluating Breath and Heart Sounds, Lippincott Williams & Wilkins, 2008.
SpringerPlus: “Post-operative Hamman’s sign: a case report.”